
One of the reasons I believe that medical malpractice lawsuits have a significant positive influence on safe patient care is the attention they bring to common problems in health care.
Sadly, in my experience, many Texas hospitals, nurses, and doctors continue to repeat the same mistakes over and over again, causing avoidable patient injuries and death. It doesn’t have to be that way, though.
For example, I recently watched a video by an obstetrician on the medical staff at the Cleveland Clinic. I’ve been familiar with this cutting-edge hospital for decades because my grandmother was treated there for Crohn’s disease. I was not surprised by what the obstetrician had to say, yet it pleased me to learn that the Cleveland Clinic is still trying to get things right.
He discussed a thorough study of closed obstetrical medical malpractice claims and the lessons they learned from those claims. Wouldn’t it be great if every hospital took the time to look into things they may have done wrong and find ways to avoid them in the future?
They took it even a step further, though. They applied the lessons learned to training for doctors and nurses that raised the bar on what they did to keep patients safe. Let’s discuss some of the things they focused on.
Not acting on abnormal fetal heart tracings
As a father of four children, I remember sitting in the labor and delivery room and watching the digital fetal heart tracing monitor for each of our kids.
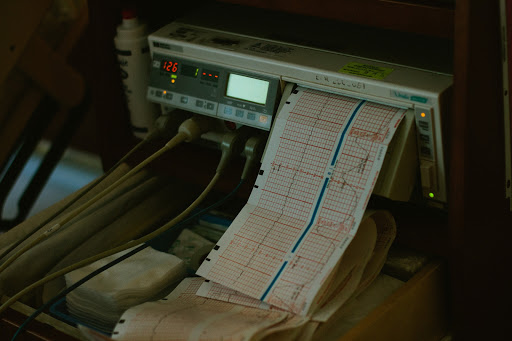
When a pregnant mother is admitted to the labor and delivery ward for monitoring, the nursing staff places two belts around her belly. The belts have sensors that are connected to an electronic fetal monitoring machine. One belt and sensor records uterine contractions. The other belt and sensor records the fetal (baby) heart rate. Over time, the heart rate is recorded as a tracing.
OB/GYN doctors and labor and delivery nurses like to see variability in the fetal heart tracing, rather than something that looks like a flat line. Good variability looks like a squiggly line, both in terms of short-term and long-term on the tracing. When there are upward bumps, or accelerations, that’s usually a good sign. When there are downward bumps, or decelerations, they may be harmless, but also could mean that the baby is going into fetal distress and needs an emergency Cesarean section (C-Section).
Doctors and nurses used to describe the fetal monitoring strip as either reassuring or non-reassuring. Although this terminology has fallen out of favor, some obstetricians and nurses still use it.
How fetal heart tracings are described
From my experience as a Houston, Texas, medical malpractice attorney, I believe it is important for doctors and nurses to use the same terminology when describing findings on an electronic fetal monitor. There’s that old jingle about how you may say tomato or potato, but the words used by healthcare providers can make a big difference in communicating whether the patient needs immediate attention.
The American College of Obstetricians and Gynecologists (ACOG) recommend the use of the three-category system to classify fetal heart rate interpretations and abnormalities.
A Category I fetal heart rate tracing is normal, with a baseline heart rate of 110-160 beats per minute, moderate variability or fluctuations in the baseline heart rate, no late variable decelerations, possible early decelerations, and possible accelerations.
A Category II fetal heart rate tracing is indeterminate, meaning it may be normal, but it may not be normal. A Category II tracing includes findings like a high heart rate (tachycardia) with variability, low heart rate (bradycardia), minimal variability, and many other factors. The medical literature shows that the baby is at risk with a Category II fetal heart rate tracing during the last two hours of labor.
Category III fetal heart rate tracings are blatantly abnormal and indicate a risk of insufficient oxygen (hypoxia) to the baby and possible acidemia (a low blood pH). With these fetal heart rate tracings, it is a medical emergency and the baby should be delivered by C-Section as quickly as possible.
Looking out for shoulder dystocia
Shoulder dystocia is a dangerous complication of pregnancy that occurs when, after the baby’s head is delivered, the front part of the shoulder gets caught above the mother’s pubic bone. In other words, the baby’s head is delivered, but the rest of the body is stuck because the shoulders cannot come out. This is an obstetrical emergency.
While OB/GYN doctors often do not discover shoulder dystocia after labor has begun, there are well-known risk factors. A pregnant mom and her baby have an increased risk of shoulder dystocia if:
· The baby is very large. Healthcare providers call this macrosomia.
· The mom is obese or has diabetes.
· The mom is carrying more than one baby.
· The delivery is past the baby’s due date.
Doctors can use ultrasound as an additional tool to identify babies that are at risk for a larger size at delivery (gestational size) and offer C-Section delivery as a safe alternative to vaginal birth.
Maternal hemorrhaging
The rate of maternal death (mothers dying) from post-partum and massive hemorrhages during or after labor and delivery is on the rise in America. What’s shocking to me about this is that, at the same time, those rates are going down virtually everywhere else in the world.
Hospitals and labor and delivery units can help address this serious and significant risk in several ways:
· Identify and treat patients at risk for hemorrhaging.
· Nurses should measure and document maternal blood and volume loss.
· Hospitals should have policies, procedures, and protocols in place for blood transfusions.
· Hospitals should have transfusion carts and pharmaceutical agents immediately available in a labor and delivery unit.
We are here to help
If you or a loved one has been seriously injured or even died because of poor OB/GYN, labor and delivery, or hospital care, then the experienced medical malpractice attorneys at Painter Law Firm, in Houston, Texas, are here to help. Click here to send us a confidential email via our “Contact Us” form or call us at 281-580-8800.
All consultations are free, and, because we only represent clients on a contingency fee, you will owe us nothing unless we win your case. We handle cases in the Houston area and all over Texas. We are currently working on medical malpractice lawsuits in Houston, The Woodlands, Sugar Land, Conroe, Dallas, Austin, San Antonio, Corpus Christi, Bryan/College Station, and Waco.
__________
Robert Painter is a medical malpractice attorney at Painter Law Firm PLLC, in Houston, Texas. He is a former hospital administrator who represents patients and family members in medical negligence and wrongful death lawsuits against hospitals, physicians, surgeons, anesthesiologists, and other healthcare providers. A member of the board of directors of the Houston Bar Association, he was honored, in 2018, by H Texas as one of Houston’s top lawyers. Also, in 2018, the Better Business Bureau recognized Painter Law Firm PLLC with its Award of Distinction.



